 |
| From Kevin Boyd |
The modern epidemic of obesity is been driven largely by a change in our diets in particularly the ubiquitous consumption of processed and ultra-processed foods and the large increase in sugar (sucrose) consumption. Prior to the Victorian era, sugar was not a dietary staple and we tended to eat large quantities of unprocessed foods. Eating unprocessed foods meant we had to work hard at chewing food, which created the stimulus for our mandibles and faces to develop. Eating processed foods means our mandibles and face have gotten smaller and has resulted in an epidemic of malocclusion and impacted wisdom teeth. This also resulted in our tongues being too big for our smaller mouths and this has resulted in our nasopharyngeal space becoming relatively smaller. The result of all of this is that obstructive sleep apnoea (OSA) is now commonly seen in children with malocclusion syndromes.
This is important because OSA results in the brain becoming intermittently hypoxic and disrupted sleep us affecting the normal physiology of the brain. We need good quality sleep to consolidate memories and for the glymphatic system to clear away the intracellular debris. Poor sleep quality is creating the substrate for an unhealthy brain from a very young age and unhealthy brains are primed to degenerate faster and earlier and may be contributing to the rise in all-cause dementia.
The anatomical changes in the mandible and face underlying the rising incidence of sleep apnoea is not the only factor affecting sleep quality at a population level. Light and noise pollution, screen addiction and many other factors are affecting sleep quality at a population level. I am therefore proposing that we need to look into sleep deprivation at a population level as an important modifiable risk factor for all-cause dementia. The question is how do we go about doing this?
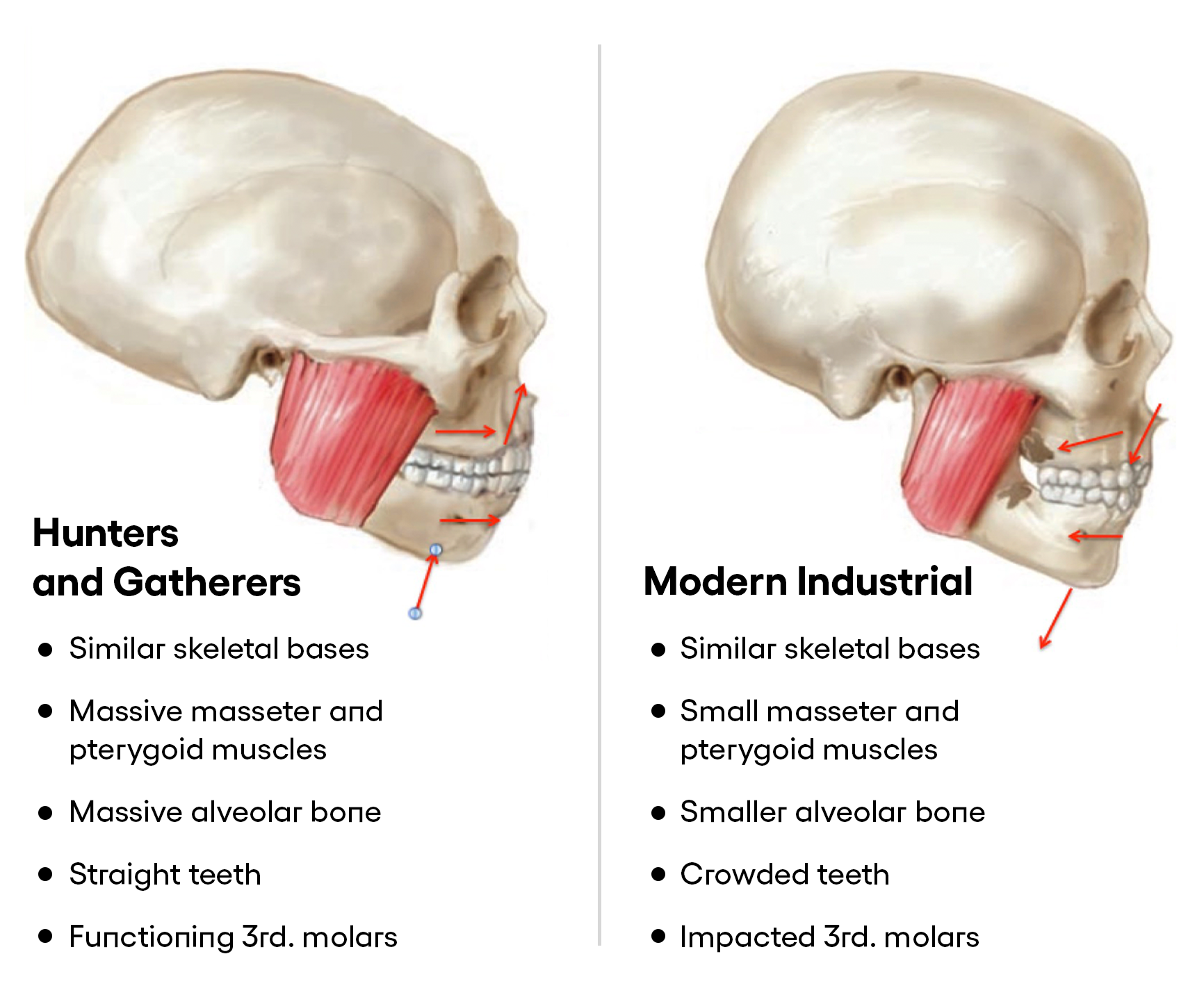 |
| Picture from Kevin Boyd |
Kevin Boyd. Darwinian dentistry part 1: An Evolutionary Perspective on the Etiology of Malocclusion. JAOS Nov/Dec 2011
Comments
Post a Comment